How faecal transplantation is gaining credibility

Many find the idea of faecal, or poo transplants disgusting. However a growing body of evidence suggests this could be a lifesaver, as Bryn Nelson reports.
This is how far a mother will go.
Your daughter has been sick for more than four years with a severe autoimmune disease that has left her colon raw with bloody ulcers. After multiple doctors and drugs have failed, you are frantic for her to get better. Then you send her disease into remission, virtually overnight, with a single act of love. “Who wouldn’t do that for their daughter?” you say. It’s like a miracle, you say. “An overnight magic wand.”
You’ve agreed to do it again – twice – for strangers. You’ve seen first-hand how effective it can be and you felt so badly for the patients and their families. Had you donated blood or plasma, no one would blink. But this? You can’t tell anyone else about this because of how they might react.
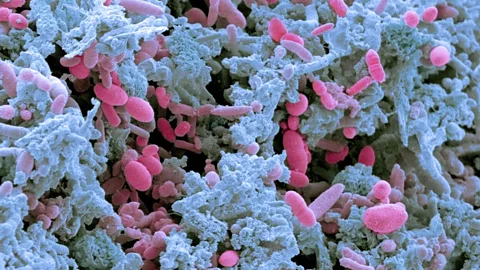
There are more like you, men and women who have given their loved ones a remarkable reprieve from a group of chronic conditions known as inflammatory bowel disease. There are many more who have cured patients of a potentially fatal bacterium known as Clostridium difficile. This microbe can persist in a cocoon-like spore for up to five months, impervious to nearly everything except bleach. It is fast becoming resistant to every antibiotic thrown at it.
You insist on “Marion” as a pseudonym. You say of your daughter’s therapy: “I don’t talk with anybody about it. I’ve told people that we replaced her…” and you pause, “unhealthy bacteria with healthy bacteria. I didn’t go into specifics.”
Here are the specifics: you were the donor in a faecal microbiota transplant. You gave your daughter your poo.
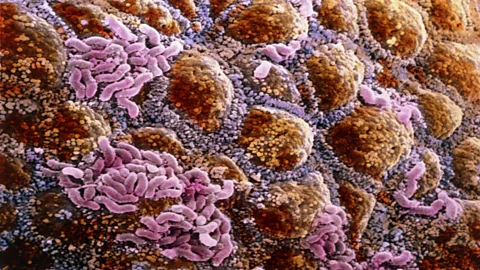
Poo is a decidedly imperfect delivery vehicle for a medical therapy. It’s messy. It stinks. It’s inconsistent, not to mention a regulatory nightmare. But it can be incredibly potent. A classic study of nine healthy British volunteers found that bacteria accounted for more than half of the mass of their faecal solids. That astonishing concentration of microorganisms, both living and dead, makes sense when you consider that the microbial colonists inhabiting our gastrointestinal tract outnumber our own cells roughly three to one, on recent estimates.
In the ideal conditions of the human gut, a thriving ecosystem of 1,000 or more bacterial species that rivals the complexity of a rainforest has co-evolved with us. This microscopic jungle is constantly adapting in response to our diet, antibiotic use and other environmental influences. As the science has progressed, researchers are now comparing the entire collection of microbial inhabitants of the human gut, our microbiome, to a “hidden metabolic organ”. Scientists have linked disruptions to this organ, a condition known as dysbiosis, to everything from inflammatory bowel disease and high blood pressure to diabetes and obesity.
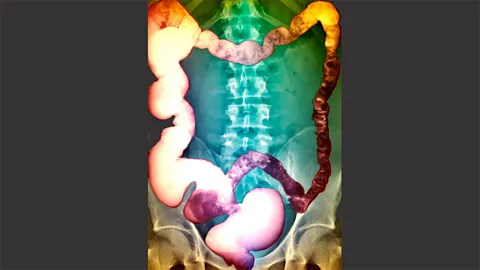
Viewed in this light, a faecal microbiota transplant is nothing more than an attempt to reseed an intestinal tract, often after antibiotics have killed off the native flora that might have kept invasive species at bay. No other medical therapy can claim such a high cure rate for the infection widely known as C. diff.
Sudden killer
Some doctors have likened the recoveries of desperately ill patients to those seen with anti-HIV protease inhibitors in the mid-1990s. After the Mayo Clinic in Scottsdale, Arizona, performed its first faecal microbiota transplant in 2011, a patient who had been bed-ridden for weeks left the hospital 24 hours later. And in 2013, researchers in the Netherlands halted a landmark C. diff. clinical trial early for ethical reasons when they saw that the overall cure rate of 94% with donor faeces had far outpaced the 31% cured with the antibiotic vancomycin.
Yet few other interventions elicit such disgust, revulsion and ridicule. Chronicling a potential advance by a team of Canadian scientists, one newspaper account warned readers: “Hold your nose and don’t spit out your coffee”.
What’s behind this knee-jerk aversion? Perhaps, as one epidemiologist believes, it’s the voice of our evolutionary ancestors, warning us away from a major source of parasites and other pathogens. Perhaps, says another researcher, it’s the fading of an agrarian life that equated manure with opportunity, whose cultural influence is now drowned out by public health warnings of diarrhoea-borne epidemics in towns and cities.
With the last lines of antibiotic defence beginning to crumble, however, getting past the cognitive dissonance of healthy poo as powerful curative could be a matter of life or death for tens of thousands of patients.
This is how bad a C. diff. infection can be. Thursday morning, she’s a healthy 56-year-old kindergarten teacher. She has a bad back from decades working as a waitress, sure, and she smoked before quitting in her 30s when she was raising two boys on her own. The chronic inflammation in her shoulder occasionally flares and she’s put on a few pounds over the years, but she’s a typical mother from a big Irish Catholic family in Brooklyn. She has low blood pressure. She’s studying for a Master’s degree in education.
She’s as tough as nails, her sons say. She doesn’t feel well after school, though, so she goes to bed early. Then the diarrhoea begins, at 4am, with a sudden urgency. She takes her first sick day in memory. Her sons bring her Gatorade, and she’s still herself on the outside, despite being weak and tired and pale. Only something horrible is happening on the inside, made worse by the strong anti-diarrhoeal drugs that her doctor prescribed. Her intestines are steeping in a toxic stew released by millions of proliferating bacteria.
By Tuesday evening, she’s the sickest patient in the hospital. She’s craving a Diet Pepsi, but her infection has progressed so far that she has toxic megacolon: her large intestine is dying. An unapologetically frank surgeon will remove it in a last-ditch attempt to save her life. She’s going into septic shock. Dozens of friends and family members crowd into the waiting room in a stunned vigil.
And it won’t be enough. By Wednesday evening, at 7.20pm, Peggy Lillis will be gone, leaving her reeling sons to wonder how she could have died so quickly from something they had never heard of.
Deadly infection
Perhaps Peggy contracted the deadly infection in the nearby nursing home where she periodically visited her godmother. Perhaps it was from the dentist’s office, where she underwent a root canal, was treated for an abscess and was prescribed clindamycin, a broad-spectrum antibiotic that can profoundly alter the gut microbiome and clear the way for C. diff.
The infection progressed so quickly that a faecal transplant – even if her sons had heard of it – may not have helped. “But I think the key thing here,” says her oldest son, Christian, “is that the disease itself and our ability to raise awareness of it and talk about it, identify it, prevent it, treat it, is all complicated by the fact that we don’t want to talk about shit.”

In 2010, Christian and his brother, Liam, co-founded the Peggy Lillis Memorial Foundation to focus more attention on an infection that has long outgrown its reputation as a nuisance in hospitals and nursing homes. “To me, it’s a really big public health crisis and one that we’re not talking about,” Christian says.
Ice-cream cartons
The first known record of faecal transplants dates back to fourth-century China, when a doctor named Ge Hong included several mentions in his ambitious collection of therapeutic formulas called Handy Therapy for Emergencies. Ge dutifully described how to treat patients with food poisoning or severe diarrhoea by feeding them a faecal suspension bluntly named “solution of stool”.
Just over a century ago, in 1910, theJournal of Advanced Therapeutics reported briefly on a new technique for treating “chronic intestinal putrefactions”. It described how a doctor had treated the intestinal disorder by injecting Bacillus bacteria into the rectum of each patient every four days, leading to a noticeable shift in the resident bacterial population.
Nearly 50 years later, Ben Eiseman, Chief of Surgery at the Denver Veterans Administration Hospital, used faecal enemas to cure three men and one woman of a life-threatening inflammatory condition called pseudomembranous enterocolitis. Amid the dry clinical language of his case reports, Eiseman recorded remarkably similar outcomes for each. “There was an immediate and dramatic response by this critically ill patient to a fecal retention enema,” he noted for the first. Nevertheless, he concluded, “enteric-coated capsules might be both more aesthetic and more effective”.
An ad hoc experiment involving capsules, in fact, was already underway on the east coast of the US at the direction of a surgeon who worried that the heavy use of pre-operative antibiotics was disrupting the normal intestinal flora of his patients. In 1957, the surgeon instructed a young bacteriologist named Stanley Falkow to begin collecting stool samples from surgical patients admitted to an unnamed hospital. Falkow, now a microbiologist and immunologist at Stanford University in Palo Alto, California, recalls dividing each patient’s poo into 12 large gelatin capsules before stashing the collection in a refrigerated ice-cream carton. The patients were then sent home with a prescription of two capsules per day in an attempt to re-establish their pre-surgical intestinal microbes.
Anecdotal reports at the time suggested that enrollees in this uncontrolled clinical trial were faring better than other post-surgical patients. But Falkow writes that they probably never knew what they were ingesting. The experiment came to an abrupt end when the chief hospital administrator found out and accused him of feeding patients their own faeces.
Doctors have since developed more than half a dozen ways to transfer faecal microbes to their patients, but a more formal follow-up to Eiseman’s suggestion would have to wait another half-century.
Yuck factor
If you ask people from Burkina Faso, India and the UK what disgusts them, chances are high that their lists will all include poo. “Probably of all of the elicitors of disgust that we’ve collected from studies around the world, that’s the most universal,” says Valerie Curtis, a self-described “disgustologist” and Director of the Hygiene Centre at the London School of Hygiene and Tropical Medicine.
There’s a good reason for that “yuck factor”, she says. Researchers have identified dozens of common species of disease-causing organisms in our poo, ranging from parasites and amoebae to bacteria, fungi and viruses. For our ancestors, Curtis hypothesises, revulsion at that potent reservoir of disease may have been a matter of self-preservation. Those who didn’t stay away would have fallen ill more often, decreasing their chances of reproducing successfully.
It’s not just poo. Anything that comes out of another human body – blood, sweat, vomit, urine, semen, saliva – can elicit a fear-based feeling of disgust that it might get into yours, she says. “Because other people are the prime sources of the diseases that might make you sick, we really don’t want to have other people’s stuff inside us.” In her book, Don’t Look, Don’t Touch, Don’t Eat, Curtis argues that our inner defence mechanism probably extends to other signposts of disease: the sweaty, unkempt appearance of someone who is unwell; the smell of rotten food; the sight of rats, flies and parasitic worms.
Not all scientists are convinced that we harbour an innate predisposition to be grossed out by things like poo. Paul Rozin, Professor of Psychology at the University of Pennsylvania (widely known as Dr Disgust), led a particularly vivid exploration of the indiscriminate tastes of toddlers in a series of experiments from the 1980s. More than half of his study subjects under the age of two readily ate a dish introduced as “dog poo” – actually peanut butter with Limburger and blue cheese. Older kids, however, were less likely to gobble it up, suggesting they had since learned what not to eat.
Canadian veterinarian and epidemiologist David Waltner-Toews suggests in his own book, The Origin of Feces, that our response to poo may instead reflect a complicated and contradictory cultural history based more on geography. Whereas faeces was traditionally associated with fertiliser in rural agricultural areas, he says, it took on a more sinister role in urban centres as public health officials emphasised the very real danger of diarrhoeal diseases.
Regardless of the reasons for our collective disgust, the fear of losing a loved one may be an effective antidote. In fact, doctor after doctor agrees that most patients with a serious gastrointestinal condition – and their families – are beyond caring that a little more faeces may be involved in a therapeutic intervention; they’ve already been through far worse.
Antibiotic resistant
Catherine Duff is deathly afraid of two things: public speaking and crickets. Poo, however, has long since ceased to disgust her. “That dissipates so quickly when you’re dying,” she says. Since 2005, she has had C. diff. eight times. The first six times, it responded to antibiotics. Then it didn’t. “My colorectal surgeon gave me the choice of having my colon removed or dying,” says Catherine, 58, from Carmel, Indiana. She had already lost a third of her colon and wasn’t about to give up any more.
With every bout of diarrhoea and vomiting, she felt the life draining out of her. “I had basically resigned myself to the fact that I was going to die.” Then one of her three daughters, a corporate tax attorney, came across the research of an Australian gastroenterologist named Thomas Borody. His group was recording astonishing results in C. diff. patients with a therapy called faecal transplant.
Catherine read everything she could and brought the printouts to her doctors. By then, she had eight specialists. Only two, an infectious disease expert and a gastroenterologist, had ever heard of the technique. Neither was willing to try it.
And so in April 2012, Catherine became part of a burgeoning DIY movement born out of necessity. Her husband, John, a retired submarine commander who had frequently spent months at a time submerged with 180 other men, readily agreed to be her faecal donor. “Nothing grosses him out,” she says. They convinced her gastroenterologist to at least have John’s poo screened for pathogens, and then found a recipe and protocol on the internet.
Catherine recalls taking the enema at 4pm. “By 7, I felt good,” she says. “It was almost miraculous how quickly I felt better.” The next morning, she took a shower and got dressed, put on make-up and went downstairs for breakfast, “things I hadn’t done in months,” she says.
Six months later, she had to undergo emergency surgery to correct a spinal cord compression caused by an old horseback riding accident. She came down with her eighth case of C. diff. before she left the hospital. But this time was different. This time, her colorectal surgeon agreed to try a faecal transplant using a colonoscopy – delivering the poo through a long, flexible tube inserted the length of her colon – and she became the first patient in the state of Indiana to undergo the procedure at a medical facility. “By the time I woke up from the sedation, I felt fine,” she says.
Officials at the US Food and Drug Administration (FDA) were increasingly feeling otherwise. Struggling over how to regulate the procedure, they labelled it a drug instead of a transplant in April 2013, a move that dismayed patient advocates and sharply curtailed the fledgling field. Providers wanting to continue treating patients would have to file an Investigational New Drug application, an arduous and time-intensive requirement that most individual physicians were ill-equipped to meet.
Lone voice
A month later, the FDA hosted a public two-day workshop on the therapy in Bethesda, Maryland. Catherine, who had just launched the Fecal Transplant Foundation to connect patients with providers and encourage more doctors to offer the treatment, was one of 150 participants. When she scanned the list of attendees, she saw that she was the only patient. Midway through the meeting, she realised there would be no discussion about the impact from a patient’s perspective, and she knew she had to do something. So she wrote an impromptu speech on her iPad over lunch and tearfully begged the moderator to let her talk during the Friday afternoon session.
Just the thought of speaking to the entire group made her hyperventilate. But she signalled the moderator, as he had instructed, and her microphone lit up. Red. She began to tell her story, haltingly. “I was crying. I was so emotional and I was so scared.” She didn’t finish her speech, but it didn’t matter by then. She received a standing ovation from the doctors in the room. Afterwards, she found herself at the end of a reception line. “All of these doctors lined up to introduce themselves and to thank me,” she says. Within a few weeks, she had assembled the majority of her foundation’s board of directors and board of advisers.
Perhaps Catherine’s testimony helped sway the FDA. Perhaps it was the deluge of bad press that caught the agency off-guard as it struggled to balance the growing evidence of benefits with a highly variable and virtually unregulated practice that had flown beneath the radar. On 18 June 2013, the FDA bowed to pressure and partially reversed course, agreeing to exercise “enforcement discretion” for faecal microbiota transplants used to treat C. diff infections that weren’t responding to standard therapy. They wouldn’t be FDA-approved, in other words, but neither would they be prohibited.
Since the small victory, Catherine and her foundation have continued to push for more faecal microbiota transplant (FMT) clinical trials aimed at other digestive disorders, more research funding and more public awareness and education. She and a few board members who share her sense of humour have also begun crafting slogans that might eventually adorn T-shirts or sweatshirts. Her favourites? “Poop is the Sh*t!” and “Give a sh*t. Donate to the Fecal Transplant Foundation.” Her site also features an FMT awareness ribbon. It’s brown.
“It is what it is,” she says with a laugh. “There’s no way around what we’re talking about or what we’re dealing with.”
Despite the ubiquity of home remedies, including Catherine’s first DIY faecal transplant, she stresses that a medically supervised procedure is far more preferable, due to the potential for disaster in patients who do not properly screen their donors. Because so many patients are still struggling to find doctors willing to perform a transplant, however, Catherine is hoping to develop a more comprehensive online database of providers who can help.
‘You’ve got to be kidding’
The unassuming one-storey office building on the periphery of the Wellswood neighbourhood in Tampa, Florida – a discreet concrete box with windows constructed from privacy glass blocks – houses two gastroenterologist practices. One of them, RDS Infusions, is among the few places in the entire Southeastern US where people with C. diff. can go for treatment. The process begins at an endoscopy centre less than a mile away, where donor poo is inserted into sedated patients: up one end through a colonoscope and down the other through an endoscope that extends past the throat and stomach to the jejunum – the midsection of the small intestine.
Among the 60 or so C. diff. patients that have followed his directives, R David Shepard, a gastroenterologist in Tampa, says he hasn’t had a failure yet. Until the FDA forced him to put his ulcerative colitis programme on hold, he had achieved a success rate of about 70% for that condition, he says. Marion’s daughter was the first.
Cautious and unfailingly polite, Shephard describes his foray into a therapeutic field that he, like many other doctors, initially dismissed.“The thought of it was basically one of disgust and ‘Oh, I’ll never do that. You’ve got to be kidding’.”
Elaine Petrof, an infectious-disease specialist at Queen’s University and Kingston General Hospital in Ontario, says doctors in her specialty are often conditioned to associate infections with germs that must be eliminated. “Just conceptually speaking, pouring sewage into people doesn’t seem like a good idea, right?” she says.
The technique lingered on the margins of accepted medical practice for years because there simply wasn’t a great need for it, says Alexander Khoruts, a gastroenterologist and immunologist at the University of Minnesota in Minneapolis. That changed within the last decade, when C. diff. became an epidemic and a more virulent strain emerged from Quebec. Doctors now routinely encounter patients whose infections have stopped responding to all antibiotics.
For Petrof, the turning point came in 2009. After a woman’s recurrent C. diff. infection stopped responding to antibiotics, she began bouncing in and out of the intensive care unit. Every day, the patient’s relatives asked Petrof to consider a faecal transplant. “I thought, ‘This is crazy’,” she recalls. Then they brought her a bucket of poo.
“What completely floored me was the fact that within less than 72 hours, this patient, who had been having over a dozen bowel movements a day, basically completely turned around and at the end of the week walked out of the hospital,” Petrof says.
Ancestor hunt
Although most providers haven’t published their overall success rates, their self-reported results are surprisingly similar, and consistent with what published reports there are. Khoruts says he has achieved a success rate of about 90% after one infusion, 99% after two. Colleen Kelly, a gastroenterologist with the Women’s Medicine Collaborative in Providence, Rhode Island, has performed the procedure on 130 patients with recurrent C. diff., with a success rate of about 95%. Most of the transplants have taken after just one attempt.
For a relatively simple bacterial infection, Petrof says, the potential remedy may be fairly straightforward. “With recurrent C. diff. what you’ve done is you’ve basically torched the forest,” she says. Nearly everything has been killed off by the antibiotics, leaving very low bacterial diversity. “So the C. diff. can just take root and grow.” Adding back almost any other flora – the equivalent of planting seedlings in the dirt – could help the ecosystem keep interloping pathogens at bay.
For more complicated conditions, though, a simple faecal transplant may not be enough, at least with donors from the Western world. One hypothesis suggests that people in lower-income countries might harbour more diverse bacterial populations in their guts than those who have grown up in a more sterile, antibiotic-rich environment. And in fact, a 2012 study found that residents of Venezuela’s Amazonas State and rural Malawi had markedly more diverse gut microbiomes than people living in three US metropolitan areas. Scientists have already raised the idea that a rise in allergies and autoimmunity in industrialised nations may derive from a kind of collective defect of reduced microbial diversity.
“We cannot find people who’ve never been on antibiotics,” Khoruts says of his donors. For complex autoimmune diseases such as ulcerative colitis, faecal transplants may offer only a partial solution. And with some data suggesting that susceptibility may be linked in part to past antibiotic exposure, perhaps no Western donor can provide the microbes needed to fully reseed the gut.
Khoruts says it may be necessary to seek out ancestral microbial communities – the ones all humans hosted before the advent of the antibiotic era – within people in Africa or the Amazon. “It’s just a disappearing resource,” he says.
Thomas Borody, founder and Director of the Centre for Digestive Diseases in Sydney and a pioneer in the faecal transplant field, finds some merit in the notion that we should seek out a more natural human microbiome. Any donor-screening process, though, would have to account for endemic parasites and pathogens. And researchers, he says, still know very little about the components of this complex and variable organ that may derive its power not only from bacteria but also from fungi and viruses such as bacteria-infecting bacteriophages.
‘Everybody giggles’
Providers repeatedly stress the importance of careful donor screening. If an untested donor passed on a significant infection or condition, it could be devastating to the field as well as the recipient. With a growing body of evidence linking the microbiome to obesity, diabetes and allergies, Khoruts also worries about the potential long-term impacts of poo from a donor with those conditions. “At this point, I think science tells us to be very cautious with this material,” he says.
Building up a bank of super-donors has not been easy. Given the rigid selection criteria, Khoruts has disqualified about 95% of respondents. “It turns out that healthy people are rare,” he says. So far, 17 volunteers have participated in his programme, but only 10 are still actively donating.
OpenBiome, a new nonprofit organisation based at the Massachusetts Institute of Technology, is trying to help fill the void by providing pre-screened, filtered and frozen poo at $250 a pop. Launched in September 2013, the bank had made 214 deliveries to 24 clinics in a dozen US states and the Canadian province of British Columbia by the first week of April 2014. Based on early, unpublished results from 25 transplants, 23 succeeded in treating recurrent C. diff., according to co-founder and Executive Director James Burgess. So far, the group’s active donor pool includes just three people, all recruited through a network of friends and colleagues at MIT. Due to soaring demand, OpenBiome is hoping to double that number.
Finding donors is harder than for blood. When Khoruts screened a medical student who had responded to a flyer, she told him her classmates laughed at her. “Nobody would giggle at a blood donor, right? You could proudly put a button on, ‘I just donated’. Everybody feels good,” he says. “You do that with a stool donor, everybody giggles. It’s embarrassing. And even though this person has just saved with one donation maybe three or four lives, which is far more than any blood donor can say, they get this peer pressure.”
Poop pills
Give it a different name. Dye it blue. Disguise the smell with lavender or citrus or pine. Take it out of its normal context and administer it amid stainless steel and clean glass surfaces. To minimise those ancestral voices of disgust, Val Curtis says, poo must be made more palatable.
Curtis recalls working with clinicians who told patients to collect their faecal samples in old margarine tubs. “And I said, ‘No wonder people won’t do it. You can’t associate poo with food, you’ve got to give them something clinical to collect it in’,” she says.
The same is true for the delivery, one reason Curtis says any method that discreetly encapsulates the poo into pills is likely to prove more acceptable. “Remember that our disgust system evolved for us to detect threats outside our bodies that want to get inside our bodies,” she says. That system may spring into action if a parasite crawls across your arm. But it won’t necessarily stop you from swallowing a triple-coated pill that releases its contents only when it has reached your intestinal tract.
Despite her own success with faecal transplants, Petrof was uneasy about the “poop milkshakes” she was putting in her patients. The result of her angst has been another alternative from a more defined subset of ingredients – essentially a mix of bacterial cultures she calls synthetic stool. The cloudy white infusions have worked for two C. diff. patients in a recent proof-of-principle study.
Petrof concedes that her technique’s feasibility remains to be seen. The bacterial mix requires a finicky growing environment akin to an artificial colon, and she believes her team may have stripped down the mixture a bit too much. Health Canada’s regulatory officials have since put Petrof’s therapy on hold pending the outcome of more tests and have asked whether it’s possible to simplify her slurry even more. In the interim, she has reverted back to conducting faecal transplants.
In the US, OpenBiome and providers like Kelly have called for poo used in faecal transplants to be regulated as a tissue (like blood), not as a drug. In February 2014, however, the FDA seemed to reverse course again with a draft guidance that, among other stipulations, would require all poo to be obtained “from a donor known to either the patient or the treating licensed health care provider”.
Despite the uncertain path forward, more than a few clinicians have glimpsed the future of medicinal poo, and it is golden. Just weeks after a research team from the University of Calgary in Canada announced its own take on the faeces-filled capsule method, dubbed “poop pills” by the press, Shepard brought the new technique to Tampa. He filled 35 triple-coated capsules with donor poo and used them to successfully treat a nursing-home patient on her fourth bout of C. diff.
By the beginning of April 2014, nearly 30 faecal transplant clinical trials were underway around the world. Roughly half were aimed at C. diff., including two testing the therapy in combination with vancomycin, and another multi-centre trial evaluating the effectiveness of fresh versus frozen donor poo.
As the therapy becomes more widely established, via something akin to a “poop pill” or “crapsule”, perhaps the infectious pool of C. diff. patients may start to dwindle. More clinicians, then, might feel emboldened to explore how our bowel flora may affect not only the gastrointestinal system but also the immune and neurological systems. At least a dozen trials are now investigating whether faecal transplants can help treat some form of inflammatory bowel disease, be it Crohn’s disease or ulcerative colitis. Another is looking into type 2 diabetes, and one is even using lean donors to test faecal transplants on patients with metabolic syndrome. Researchers say it won’t be long before they’re joined by studies investigating whether the therapy might aid diseases like multiple sclerosis and autism.
Despite all the ridicule and aversion and shame, we can no longer deny the emerging power of poo. Perhaps it’s time to push past the disgust and start giving the proverbial. And doing so proudly.
This is an edited version of an article originally published by Mosaic, and is reproduced under a Creative Commons licence. For more Mosaicarticles click here.If you would like to comment on this, or anything else you have seen on Future, head over to our Facebook or Google+ page, or message us on Twitter.
